This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Date of admission:2/2/2022
A 30 yrs old female patient presented to OPD with a complain of red coloured painful lesions all over the body.
History of present illness:
Patient was apparently asymptomatic 1year back then she observed pain initially over skin of left leg following which she noticed a small nodular lesion initially small with reddish discoloration , with burning sensation and non itching and they had been progressively grown and felt localized rise in temperature which over days healed with hyperpigmented rashes.
Intially she used ayurvedic medicine for few months even then the lesions didnot subside completely.
6 months back she developed similar non itchy lesions over both hands extending proximally and healed with hyperpigmented rash.
Pain-Nodules-burning sensation-heals with hyperpigmentation.
History of past illness:
Since 8 months she developed similar lesions on face and from 1 and half to 2 months she developed similar lesions on ears and on body currently not healed.
No history of Diabetes, hypertension,TB, Asthma
Personal history:
Diet:Mixed diet
appetite -normal
bowel and bladder - Normal
Habbits:no addiction
Not allergic to any known drugs
Family history:
No familial resemblance of similar condition in any known relatives.
General examination:
Patient is conscious coherent cooperative and we'll orientated to time and place
no pallor, icterus, cyanosis, clubbing, lymphadenopathy, oedema, dehydration.
Vitals:
temperature - afebrile
pulse rate - 82 bpm
RR - 18 cpm
BP - 130/80 mm hg
SPO2 - 98 on RA
GRBS - 117.mg %
Systemic examination:
Cvs: bilaterally symmetric chest wall .
no precordial bulge .
no thrills and no murmurs.
s1 and s2 heard
Respiratory system: bilateral air entery present ,
no wheeze,
Position of trachea- central,
CNS: patient is normal and concious .
reflexs are normal
speech - normal
power
U.L - 5/5
L.L - 5/5
TONE - normal
REFLEXES
KNEE - +
BICEP - +
TRICEP-+
ANKLE - +
BRACHIORADIALIS - +
PLANTAR - withdrawal
P/A: soft and non tender
Provisional diagnosis:
ERYTHEMA NODOSUM LEPROSUM (CUTANEOUS VASCULITIS)
Investigations:
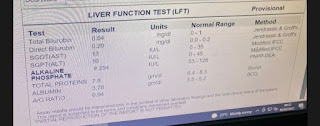
Liver function tests:
Hemogram
Complete urine examination:
ECG:
Treatment:
Topical application of fudic cream BD for 1 week.
















Comments
Post a Comment