General medicine case presentation 7
This is an online Elog book to discuss our patients de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those clinical problems with collective current best evidence based inputs.
75 year old female Came to casualty with chief complaint of involuntary movements since yesterday night .
Urinary incontinance +
Uprolling of eye balls , no tongue bite
Aphasia ( resolved)
Patient was apprantly asymptomatic 3 years ago then she had h/o CVA with monoplegia and on regular medication.
H/o HTN since 3 years and on tab amlodipine 5mg , atenolol 50 mg . H/o trauma to right lower leg associated with swelling and fever was diagnosed as cellulitis and she neglected resulting in flare up of cellulitus for which she was admitted in our hospital twice .
H/o Epilepsy 6 mon back not on any medication .
K/C/O Dm type 2 since 6 months and on tablet METFORMIN 500 MG, GLEMIPERIDE 1 MG .
HISTORY OF PRESENT ILLNESS
Patient while doing her usual household activites at around 9 - 9:30 after having dinner while she went to bed and after some time her husband heard some noises and
On waking up patient was having involuntary movements with stiffening and movement of neck to right side which lasted for about 15 min with urinary incontinence twice and was taken to local doctor gave symptomatic treatment . Husband also gave h/o aphasia and Post ictal confusion after wakeup .
PAST HISTORY
DM since 6 mon and on medication TAB.METFORMIN 500 MG , GLEMIPERIDE 1MG.
HTN since 3 years and on medication TAB. AMLODIPINE 5MG , ATENOLOL 50 MG.
PERSONAL HISTORY
Diet : Mixed
Appetite : Normal
Sleep : Adequate
Bowels : constipation
Micturition : Normal
No addictions
Drug history : non allergic for any known drugs.
Family history :No significant family history
GENERAL EXAMINATION:
Patient was conscious, coherent, cooperative NO pallor , icterus , cyanosis, clubbing , lymphadenoapthy
VITALS
BP : 90/60 MM HG
PR : 72 / MIN
RR : 18 / MIN
SPO 2 : 98% ON RA
GRBS : 188 MG %
SYSTEMIC examination
CARDIOVASCULAR SYSTEM
Inspection:
Chest wall is bilaterally symmetrical
No Precordial bulge
No visible pulsations, engorged veins,scars, sinuses
Palpation:
JVP - normal
Apex beat : felt in the left 5th intercostal space
In midclavicular line
Ausculation:
S1 ,S2 Heard
RESPIRATORY SYSTEM
Bilateral airway +
Position of trachea- central
Normal vesicular breath sounds - heard
No added sounds
PER ABDOMEN
Abdomen is soft and non tender
Bowel sounds heard
No palpable mass or free fluid
CNS :
GCS - 15/15
HMF - INTACT
SPEECH - SLURRED
SENSORY SYSTEM - INTACT
Face deviation towards left side
MOTOR SYSTEM
R L
TONE UL NORMAL NORMAL
LL NORMAL NORMAL
POWER UL 5/5 5/5
LL 5/5 5/5
REFLEXES
B T S K A
R 2+ 2+ 2+ 2+ -
L - 2+ - 2+ -
PROVISNAL DIAGNOSIS
SEIZURES UNDER EVALUATION
K/C/O CVA SINCE 3 YEARS
K/C/O DM TYPE 2 SINCE 6 MON
K/C/O HTN SINCE 3 YEARS




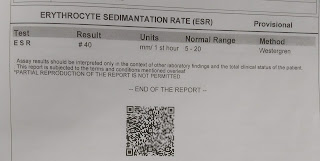
INVESTIGATIONS


Treatment plan:
- IVF 1 unit NS WITH 1 AMP OF OPTINEURON.@ 75 ML /HR
- INJ . LEVIPIL 500MG IV BD
- INJ PAN 40 MG IV OD BBF
- INJ NEOMAL IF TEMP > 101 F
- TAB. DOLO 650 MG PO SOS
- TAB . ECOSPRIN GOLD
- TAB. GLIMI M1 PO OD
- INJ HUMAN ACTRAPID INSULIN S/C
25/10/21
ICU patient
A 75 year old patient with h/o seizures.
S: Patient is feeling symptomatically better. No episode of seizures again after admission. No other complaints.
O: Patient is conscious, coherent,co operative No pallor, icterus, cyanosis, lymphadenopathy, pedel edema.
VITALS:
BP: 110/70 mmhg
PR: 78 bpm
RR: 20 cpm
Temp: afebrile to touch.
CVS: S1 AND S2 HEARD.
RS: BAE +, NVBS.
P/A: soft and non-tender.
CNS:
Patient is conscious, coherent, cooperative and is well oriented to time, place and person.
Speech is slightly slurred. Comprehension present.
Cranial nerves: intact.
Motor system :
UL. LL
- Power: R 5/5 5/5
L 5/5. 5/5
- Tone: R n n
L. n n
- Reflexes: B T S K A P
R. + + - + - flexor
L + + - + - flexor
A: Seizures under evaluation.
K/C/O old CVA in left fronto temporal region.
Old infract in right putamen
K/C/O T2 DM since 6 months.
K/C/O HTN since 3 years.
Plan of treatment:
1) IVF ( NS, RL) @ 75ML.
2) Inj. Levil 500mg iv bd.
3) Inj. PAN 40MG iv od.
4) Inj. HAI S/C premeal TID.
5) Inj. Lorazepam 2cc iv sos.
6) Inj. NEOMOL 1gm iv sos.
7) Tab. ECOSPRIN GOLD.
8) Tab. Dolo 650mg po sos.
26/10/21
AMC patient
A 75 year old patient with h/o seizures.
S: Patient is feeling symptomatically better. No episode of seizures again after admission. No other complaints.
O:Patient is conscious coherent cooperative and we'll oriented to time,place
No pallor, icterus, cyanosis, lymphadenopathy, pedel edema.
VITALS:
BP: 100/70 mmhg
PR: 78 bpm
RR: 18cpm
Temp: afebrile to touch.
CVS: S1 AND S2 HEARD.
RS: BAE +, NVBS.
P/A: soft and non-tender.
CNS:
Patient is conscious, coherent, cooperative and is well oriented to time, place and person.
Speech is slightly slurred. Comprehension present.
Cranial nerves: intact.
Motor system :
UL. LL
- Power: R 5/5 5/5
L 5/5. 5/5
- Tone: R n n
L. n n
- Reflexes: B T S K A P
R. + + - + - flexor
L + + - + - flexor
A: Seizures under evaluation.
K/C/O old CVA in left fronto temporal region.
Old infract in right putamen
K/C/O T2 DM since 6 months.
K/C/O HTN since 3 years.
Plan of treatment:
1) IVF ( NS, RL) @ 75ML.
2) Inj. Levil 500mg iv bd.
3) Inj. PAN 40MG iv od.
4) Inj. HAI S/C premeal TID.
5) Inj. Lorazepam 2cc iv sos.
6) Inj. NEOMOL 1gm iv sos.
7) Tab. ECOSPRIN GOLD.
8) Tab. Dolo 650mg po sos.



Comments
Post a Comment